
- Direct effect by the growth hormone
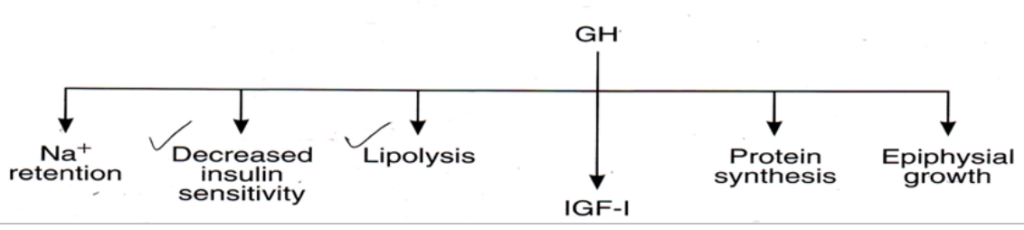
- Indirect effect- through insulin-like growth factor-I (IGF-I) or somatomedins C. It is released predominantly from the liver in response to GH. The overall functions of growth hormones are summarized in the picture below.
Metabolic effect
On carbohydrate metabolism: hyperglycemic effect
- Increase gluconeogenesis by the liver
- Decrease glucose uptake by skeletal muscle & fat
- Induced insulin resistance
- Ketogenic- it increases circulating FFA and increases ketone bodies (acetoacetate, hydroxybutyrate, and acetone)
Anabolic effect on protein metabolism
- Increase amino acid transport through the cell membrane
- Increase DNA transcription to form RNA
- Increase RNA translation
- Protein sparer
Catabolic effect on fat metabolism
- Growth hormone enhances fat utilization by stimulating triglyceride breakdown ( blood FFA).
- Fat is used for energy in preference to carbohydrates & proteins.
Hyposecretory state of growth hormone
Dwarfism
- Short stature, due to GHRH, GH, IGF-I deficiency
- Laron Dwarfism (GH insensitivity): Plasma concentration of GH normal or elevated but GH receptors are unresponsiveness.
- African Pigmies: normal plasma GH but the congenital inability to produce normal plasma somatomedin c (IGF-1).
- Psychosocial dwarfism (Kaspar Hauser syndrome): chronic abuse and neglect cause dwarfism in children.
Hypersecretory state of growth hormone
Gigantism:
- Caused by the tumor of the anterior pituitary gland before puberty.
- Epiphyseal growth plates open state.
- This leads to excessive growth of long bones
Acromegaly
- If the tumor of the anterior pituitary gland occurs after puberty
- after the epiphyses of the long bones have fused with shafts
- soft tissue continues to grow and the bones grow in thickness.
Stimuli that affect GH secretion:
- Hypoglycemia, fasting
- starvation with severe protein deficiency
- Increase circulating amino acid(protein meal)
- Decrease FFA
- Stress (exercise, trauma, excitement)